A Case for Losartan in the Management of Malignant Ascites
Last revision: 02-13-24
By Eugene L. Heyden, RN
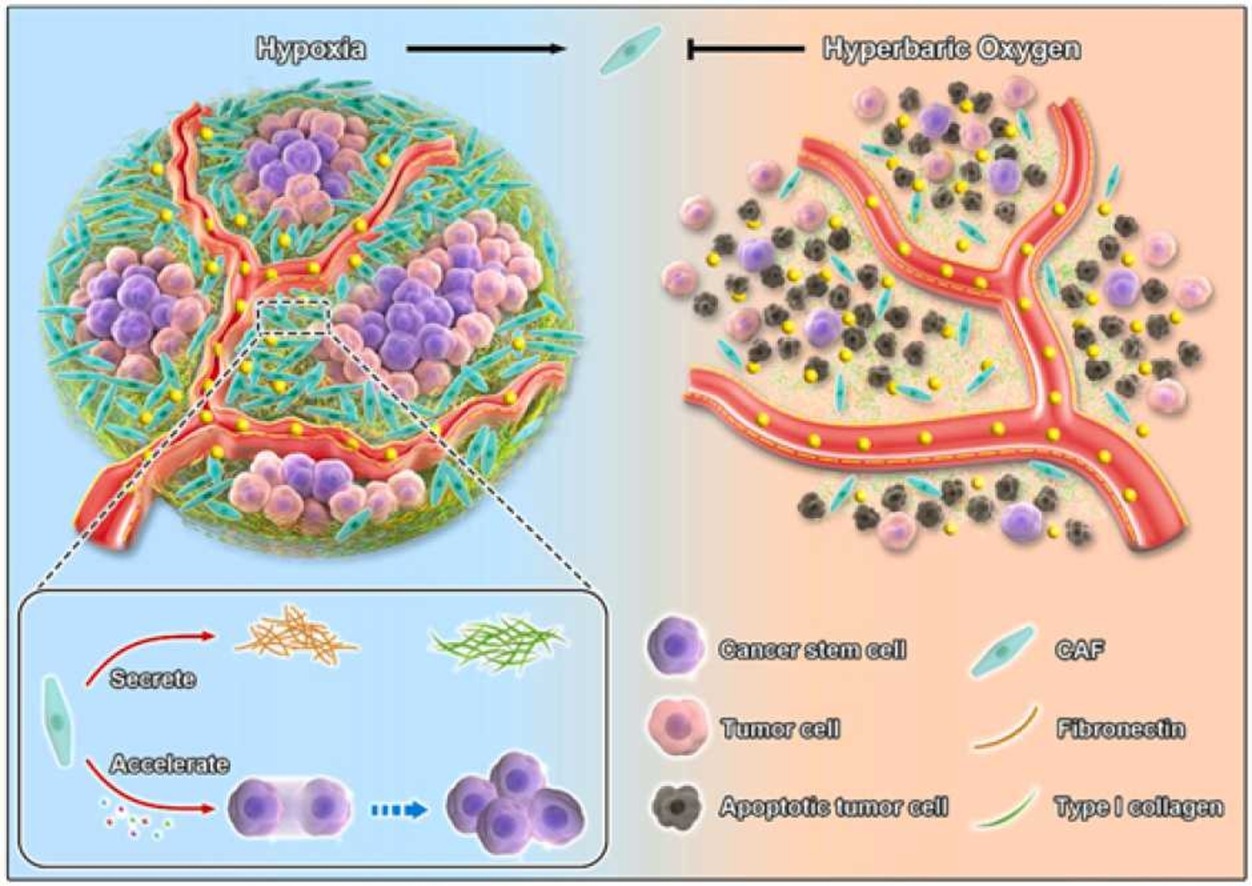
“Key to dismal clinical treatment is the unique tumor micro-environment (TME), especially abnormal tumor mechanics, associated with PDAC [pancreatic ductal adenocarcinoma]. It is well-documented that PDAC has an abundant stroma with overactivated cancer-associated fibroblasts (CAFs) and massive extracellular matrix (ECM). Together with the fast-proliferating cancer cells, extremely high solid stress is accumulated within PDAC tumor tissues, thereby compressing intra-tumoral blood vessels and deteriorating oxygen delivery. As a consequence, PDAC is featured with a severe hypoxic condition while tumor hypoxia not only promotes cancer progression but also causes resistances to various therapies.” ~ Wang et al, 2022
Relevant to our discussion, is the demonstration that hyperbaric oxygen therapy can profoundly influence the tumor microenvironment. No, I haven’t forgotten that this discussion is about losartan. We’ll get there, so please be patient.
Now regarding the tumor microenvironment, one should consider what a mess it is. It is a crowded field of tumor cells, connective tissue, cells that support tumor growth and maintenance (e.g., cancer-associated fibroblasts), and blood vessels that are deformed and ineffective at transporting oxygen and nutrients, removing waste products, and delivering therapeutics. But the tumor doesn’t mind at all. This chaotic microenvironment is how it survives and how it thrives. If you would like to see an illustration of this (actually, mandatory!), click the following link:
1-s2.0-S1748013222000858-ga1_lrg
{kind=link}
(Note: The illustration in question is from Wang et al., 2022.)
Continuing our discussion, and light of the illustration, “Hyperbaric oxygen (HBO) therapy represents one of the most effective medical treatments in overcoming tumor hypoxia and HBO has been thus used to promote antitumor efficacy of radiation therapy and photodynamic therapy (PDT) in bedside applications.” (Wang et al., 2022)
Intriguingly, with respect to pancreatic ductal adenocarcinoma, a drug called losartan can accomplish the same effects as outlined in referenced illustration.
“Alternatively, PDAC tumor mechanics has been regulated by anti-hypertension drug Losartan, which interrupts the synthesis of both collagen Ⅰ and hyaluronan in CAFs and remarkably promotes margin-negative (R0) resection rate of neoadjuvant therapy for locally advanced pancreatic cancer patients in a Phase Ⅱ clinical trial. Furthermore, Losartan has been used to normalize tumor stroma and associated with prolonged overall survival in patients with ovarian cancer and metastatic colorectal cancer. Collectively, these studies demonstrate that modulating tumor mechanics is beneficial for anticancer efficacy in not only rodent tumor models but more importantly human cancer patients.” (Wang et al, 2022, emphasis added)
Not only would losartan be helpful in addressing the “extremely high solid stress” within the tumor itself, but there is an opportunity present to use losartan to address a serious complication often encountered by the pancreatic cancer patient, namely malignant ascites—a condition commonly occurring in ovarian cancer, as well.
Remarkably, the use of losartan in ovarian cancer has demonstrated longer survival and a decrease in the degree of malignant ascites. From one study:
“Here, we report that targeting angiotensin signaling with losartan, an angiotensin receptor blocker, can reduce extracellular matrix in ovarian tumors and the associated physical barriers that normally hinder drug delivery and efficacy. These changes in the tumor microenvironment lead to improved response to chemotherapy, and, importantly, decrease ascites—a major burden for ovarian cancer patients.” (Zhao et al., 2019, emphasis added)
Aside from the issue of malignant ascites in ovarian cancer, the difference losartan can make is not inconsequential.
“. . . our retrospective analysis revealed that patients receiving angiotensin system inhibitors [e.g., Losartan] concurrently with standard treatment for ovarian cancer exhibited 30 mo longer overall survival compared with patients on other antihypertensives.” (Zhao et al., 2019, emphasis added)
The mechanisms involved with the development of ascites in ovarian cancer appear to be similar to that of other metastatic cancers such a pancreatic cancer (see Zhao et al., 2019), outlined as follows:
“The majority of patients with stage III or IV ovarian cancer develop malignant ascites and suffer from symptoms such as abdominal pressure and distension, dyspnea, bloating, pelvic pain, and bowel/bladder dysfunction. A combination of increased production of peritoneal fluid from elevated expression of tumor VEGF [vascular endothelial growth factor] and decreased drainage through diaphragmatic lymphatic channels results in the accumulation of ascites.” (Zhao et al., 2019, emphasis added)
All in all, it would seem reasonable to offer a therapeutic trial of losartan for an individual experiencing malignant ascites, in as much as
“Losartan has been shown to decrease the expression of VEGF; however, in our study, we did not observe VEGF expression change after losartan treatment. While we did not investigate it, losartan may also decrease the expression of molecules other than VEGF that are responsible for ascites formation.
“Our results suggest that in patients with relapsed or refractory ovarian cancer where chemotherapy no longer has effect on tumor burden losartan may be an option for controlling ascites, relieving symptoms and improving life quality.” (Zhao et al., 2019, emphasis added)
Accordingly, losartan administration is poised to be of substantial benefit to the patient with pancreatic cancer.
“In mouse models of breast cancer and pancreatic cancer, losartan decreased the intratumoral expression of thrombospondin-1 (THBS-1), an activator of the fibrogenic TGF-β, and significantly reduced the intratumoral collagen and hyaluronan content. As a consequence solid stress was reduced, vessel compression was alleviated, and vascular perfusion was enhanced, resulting in reduced tumor hypoxia and improved delivery and efficacy of both lowmolecular-weight drugs and nanomedicine. These studies led to a successful phase II trial of losartan combined with chemoradiation in locally advanced pancreatic cancer.” (Zhao et al., 2019, emphasis added)
“Retrospective observational cohort studies suggest that patients with pancreatic cancer who were already taking angiotensin-converting enzyme inhibitors or ARBs because of preexisting cardiovascular disease had longer survival.” (Murphy et al., 2019)
Referring again to Zaho et al., there are clear benefits to the use of losartan in cancer treatment, particularly cancers involving malignant ascites. Specifically,
- Losartan reduces mechanical stresses in solid tumors
- Losartan reduces blood vessel compression in the tumor microenvironment, leading to increased tumor perfusion and improved drug delivery
- Losartan reduces tumor hypoxia
- Losartan decreases lymphatic vessel compression, leading to increased peritoneal fluid drainage and ascites reduction
Regarding the use of losartan in clinic, there are important considerations to keep in mind:
“To use losartan as an adjunct in the treatment of cancer patients, it is important to consider dosing and treatment schedules along with potential side effects. Results from our dose- and time-dependent studies suggest a minimum of 2 wk of losartan administration before antitumor treatment. To obtain maximum effects in patients, it might be prudent to initiate losartan treatment 2 wk before and continue it during the entire antitumor treatment schedule. Because long-term losartan therapy in hypertensive patients has been shown to have limited and manageable side effects and many antitumor agents (e.g., anti-VEGF drugs) have been shown to increase blood pressure, extended losartan cotherapy could be beneficial to cancer patients. For clinical studies, we suggest treating patients with a dose of 2 mg·kg−1 ·d−1, which is similar to that used for the treatment of patients with Marfan’s syndrome.” (Diop-Frimpong et al., 2011, emphasis added)
And in one study,
“Tolerance of losartan was established during a 1-week trial dose period of 25 mg orally taken daily starting on cycle 1 day 1. If this dose was tolerated during week 1 (based on meeting or exceeding baseline minimum mean arterial pressure criterion), it was increased to 50 mg orally taken daily at cycle 1, day 8 and continued at this dose daily until the completion of cycle 8, day 14 of FOLFIRINOX treatment. Patients were monitored for drug-related hyperkalemia.” (Murphy et al., 2019)
A conclusion or two is simple to make. The off-label use of losartan should be strongly considered in the treatment of malignant ascites and perhaps prescribed early in the disease process as a measure to modify the tumor microenvironment and perhaps prevent or forestall the occurrence of malignant ascites. But in any event, time is of the essence. “In patients with pancreatic ductal adenocarcinoma (PDAC), ascites is often diagnosed late with average onset of 11 months from the time of diagnosis. Prognosis is poor after ascites development with an estimated median survival of 1.8 months from time of onset.” (Baretti et al., 2019)
Let me end with this:
“Subsequent preclinical experiments with breast and pancreatic cancer models showed losartan to reduce the amount of both collagen and hyaluronan intratumorally, resulting in decompression of tumor vessels and significantly improved perfusion. Furthermore, less hypoxia, enhanced delivery of chemotherapy, and improved overall survival were observed after losartan treatment—both for mice with breast tumors and mice with pancreatic tumors.
“Highly advantageous effects have been observed after losartan treatment, and in addition, this drug is considered safe, it is relatively inexpensive, and it is already widely prescribed as an antihypertensive agent.” (Hauge and Rofstad, 2020)
Addendum
“Currently, several ongoing clinical trials at different phases are being conducted to further study the benefit of using losartan in the treatment of pancreatic cancer (NCT04539808 in phase II, NCT03563248 in phase II and NCT04106856 in phase I).” (Rebelo et al., 2021)
Related posts: (Click image to view)
References
Baretti M, Pulluri B, Tsai HL, Blackford AL, Wolfgang CL, Laheru D, Zheng L, Herman J, Le DT, Narang AK, de Jesus-Acosta A. The significance of ascites in patients with pancreatic ductal adenocarcinoma: a case-control study. Pancreas. 2019 Apr;48(4):585. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386821/
Diop-Frimpong B, Chauhan VP, Krane S, Boucher Y, Jain RK. Losartan inhibits collagen I synthesis and improves the distribution and efficacy of nanotherapeutics in tumors. Proceedings of the National Academy of Sciences. 2011 Feb 15;108(7):2909-14. https://www.pnas.org/doi/abs/10.1073/pnas.1018892108
Hauge A, Rofstad EK. Antifibrotic therapy to normalize the tumor microenvironment. Journal of translational medicine. 2020 Dec;18:1-1. https://link.springer.com/article/10.1186/s12967-020-02376-y
Murphy JE, Wo JY, Ryan DP, Clark JW, Jiang W, Yeap BY, Drapek LC, Ly L, Baglini CV, Blaszkowsky LS, Ferrone CR. Total neoadjuvant therapy with FOLFIRINOX in combination with losartan followed by chemoradiotherapy for locally advanced pancreatic cancer: a phase 2 clinical trial. JAMA oncology. 2019 Jul 1;5(7):1020-7. https://jamanetwork.com/journals/jamaoncology/article-abstract/2734827
Rebelo R, Polónia B, Santos LL, Vasconcelos MH, Xavier CP. Drug repurposing opportunities in pancreatic ductal adenocarcinoma. Pharmaceuticals. 2021 Mar 20;14(3):280. https://www.mdpi.com/1041736”
Wang X, Ye N, Xu C, Xiao C, Zhang Z, Deng Q, Li S, Li J, Li Z, Yang X. Hyperbaric oxygen regulates tumor mechanics and augments Abraxane and gemcitabine antitumor effects against pancreatic ductal adenocarcinoma by inhibiting cancer-associated fibroblasts. Nano Today. 2022 Jun 1;44:101458. https://www.sciencedirect.com/science/article/pii/S1748013222000858
Zhao Y, Cao J, Melamed A, Worley M, Gockley A, Jones D, Nia HT, Zhang Y, Stylianopoulos T, Kumar AS, Mpekris F. Losartan treatment enhances chemotherapy efficacy and reduces ascites in ovarian cancer models by normalizing the tumor stroma. Proceedings of the National Academy of Sciences. 2019 Feb 5;116(6):2210-9. https://www.pnas.org/doi/abs/10.1073/pnas.1818357116
DISCLAIMER: This article is offered solely for informational purposes. The information contained therein and opinions expressed should be evaluated for accuracy and validity in the context of opposing data, new information, and the views and recommendations of a qualified health care professional, and not to be substituted for professional judgment and guidance or to provide a reason to neglect or delay appropriate medical care for self or for others. It is the reader and reader only who bears the responsibility for any actions that could be construed as being a response to the information presented. The statements and opinions expressed by the author have not been reviewed or approved by the FDA or by any other authoritative body, nor is the author endorsing any product or specific therapy mentioned. This article and the opinions contained therein are offered to the reader to broaden his or her understanding of the issues discussed and to help identify options that may be suitable for the individual to pursue, on behalf of self or others, under approval and direction of a qualified physician or medical team member. All questions of a medical nature which arise from reading this article should be directed at qualified health care professional. There are no guarantees that a suggested website and internal links are safe to visit or open or are currently available.
Copyright © 2023 Eugene L. Heyden, RN
All Rights Reserved
